Houston stands proudly as a global leader and top-ranked hub for healthcare, a testament to its sprawling medical center and innovative practices. The Texas Medical Center, recognized as the world’s largest medical complex, treats 4.8 million patients annually across its 42 nonprofit institutions. Yet, even in such a distinguished environment, pain management practices face unique challenges, particularly concerning compliance and revenue cycle management. Recent data indicates a concerning trend: audit rates for pain management practices are on the rise nationwide, underscoring the critical need for meticulous billing and coding.
Against this backdrop, the upcoming 2024-2025 Evaluation and Management (E/M) coding changes are not merely administrative adjustments; they are pivotal updates that will significantly impact compliance and revenue for every pain management clinic in the city. With Medicare Advantage enrollment reaching 50.2% penetration in Texas, representing a substantial portion of the patient base, accurate code selection has direct financial implications. The CMS Region 6 office in Dallas, which oversees Texas healthcare compliance, has intensified scrutiny on billing accuracy across specialties.
Navigating these complexities correctly is essential for financial stability and sustained patient care. This guide will delve into these critical E/M Coding Pain Management Houston updates, providing actionable insights rooted in the latest 2025 AMA guidelines and compliance bulletins from CMS. Understanding these shifts is paramount for safeguarding your revenue and ensuring seamless operations. For a broader perspective on optimizing your practice’s operations and financial health, explore our resources on Essential Backoffice Solutions for Healthcare Practices.
2024-2025 E/M Coding Changes: What Houston Pain Clinics Must Know
The landscape of medical coding is continuously evolving, and the changes slated for 2024-2025, particularly impacting E/M services, demand immediate attention from Houston pain management clinics. These Medical Coding Updates Houston represent a significant shift from previous coding methodologies, which often relied heavily on physical exam components and less on the cognitive work involved in patient care.
Specifically, the CPT 2024 updates introduced crucial modifications to time-based reporting, refining how patient encounters are documented. Looking ahead, 2025 will solidify the dominance of Medical Decision Making (MDM) as the primary determinant for E/M service levels across most outpatient settings, marking a decisive departure from the pre-2023 reliance on documentation volume. This evolution is particularly relevant in Houston, where the city’s 44.1% Hispanic/Latino population presents unique documentation challenges, and where Medicare Advantage enrollment significantly influences coding accuracy and financial implications for practices.
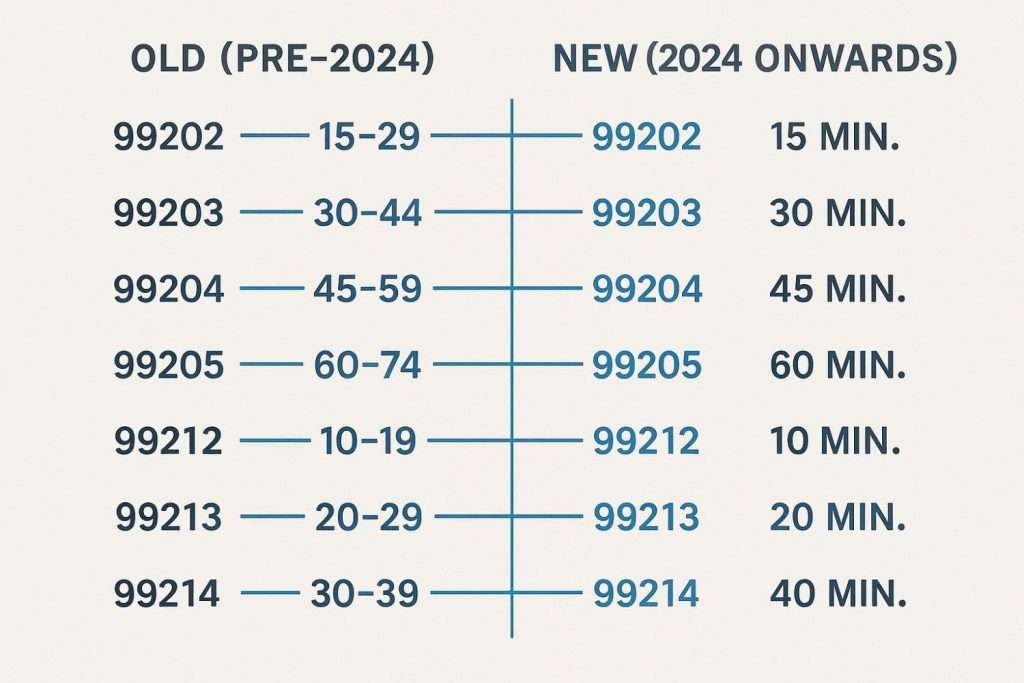
Change 1: Single Time Thresholds Replace Ranges (CPT 2024)
Effective January 1, 2024, the Centers for Medicare & Medicaid Services (CMS) finalized changes to E/M codes for office or other outpatient visits by establishing single time thresholds, replacing the previously broad time ranges. For instance:
- CPT code 99202 now has a floor of 15 minutes
- CPT code 99203 requires a minimum of 30 minutes
- CPT code 99204 specifies 45 minutes, and so on
This refinement means that providers must accurately document the total time spent on the date of the encounter, encompassing all face-to-face and non-face-to-face activities related to the patient’s care. Consider a Houston-specific example: a chronic pain consultation with a new patient that involves 44 minutes of total time. Under the old system, this might have been billed as 99203 (30-44 minutes). However, with the 2024 update, 44 minutes now dictates that the visit must be billed as 99204 (requiring a minimum of 45 minutes), assuming the visit’s content supports that level.
Failing to meet the specific threshold, even by a minute, means downcoding. This precise documentation requirement is crucial for pain management practices; explore our insights on medical billing and coding for effective management.
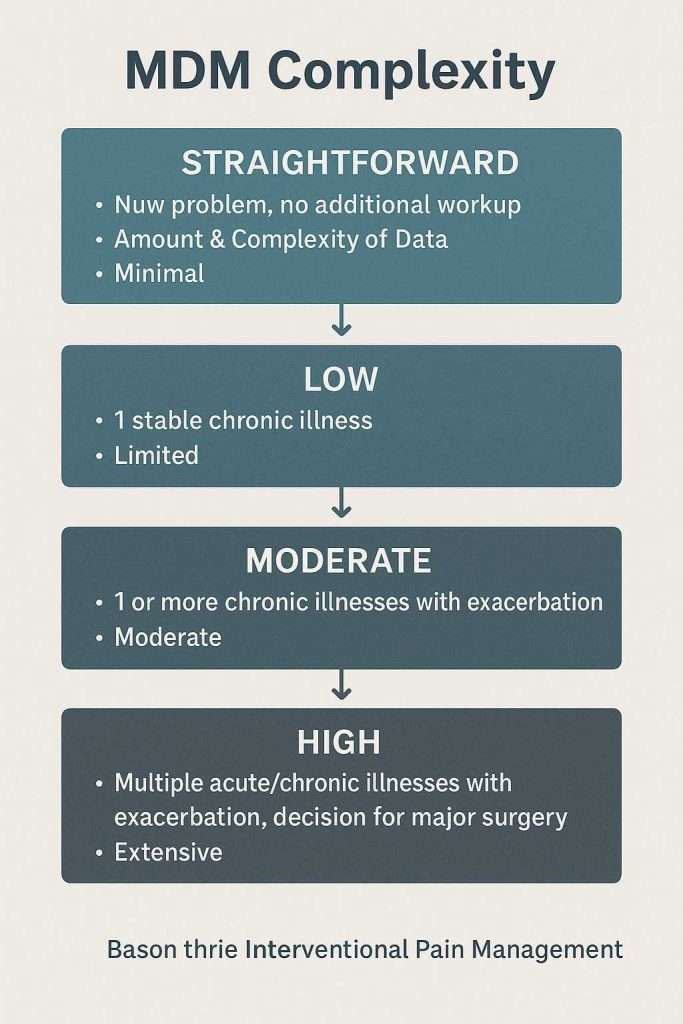
Change 2: Medical Decision Making (MDM) Becomes Primary in 2025
While time thresholds were refined in 2024, 2025 will solidify Medical Decision Making (MDM) as the dominant factor for selecting E/M service levels for office and other outpatient visits. This change emphasizes the complexity of thought involved in diagnosing and managing a patient’s condition, rather than simply the time spent or the volume of documentation. The MDM tiers (straightforward, low, moderate, and high complexity) are now determined by three core elements:
- Number and Complexity of Problems Addressed: How many and how difficult are the patient’s active problems?
- Amount and/or Complexity of Data to be Reviewed and Analyzed: This includes test results, external records, and independent historian input
- Risk of Complications and/or Morbidity or Mortality of Patient Management: This considers the risk associated with the management options selected
Medical Decision Making complexity flowchart for interventional pain management procedures
For a Houston pain management practice, consider coding a post-laminectomy follow-up. Under the new MDM-driven rules, the code selection will pivot on the complexities arising from the patient’s comorbidities (e.g., diabetes, cardiac issues), the nuanced assessment of their pain management regimen (e.g., opioid weaning, polypharmacy), and the overall risk of further complications or treatment side effects, rather than just the duration of the visit.
This shift demands a deeper understanding of MDM elements to accurately capture the visit’s complexity and ensure appropriate Pain Management Billing. This is particularly relevant for common Houston patient profiles, such as oil industry workers who may present with intricate chronic pain conditions. Research shows that 24% of petrochemical and petroleum refinery workers suffer from chronic pain, with headache being the most frequent complaint (29.9%), often compounded by polypharmacy issues requiring a higher level of medical decision making.
Change 3: New Add-On Code G2211 for Complex Care
A significant addition that directly benefits pain management practices is the new Medicare add-on code G2211, effective January 1, 2024. This code is designed to account for the additional resource costs associated with providing longitudinal, complex care for a single serious or complex chronic condition. The national reimbursement rate for G2211 is approximately $16.05.
G2211 is applicable when a practitioner is providing comprehensive, continuous care for a patient with a single, serious, and complex chronic condition, typically seen over an extended period. For pain management, this often involves conditions like chronic neuropathic pain, complex regional pain syndrome (CRPS), or persistent post-surgical pain requiring ongoing management.
The American Society of Regional Anesthesia and Pain Medicine (ASRA Pain Medicine) released detailed guidance in 2024 on the specific documentation requirements for G2211, emphasizing the need to clearly articulate the ongoing, comprehensive nature of care for a single complex condition. This add-on code is a crucial update in the broader landscape of Medical Coding Updates Houston, allowing practices to better reflect the true value of their longitudinal care.
For expert assistance in navigating these complex coding changes and ensuring compliance, consider reaching out to our specialized Houston medical billing and coding services.
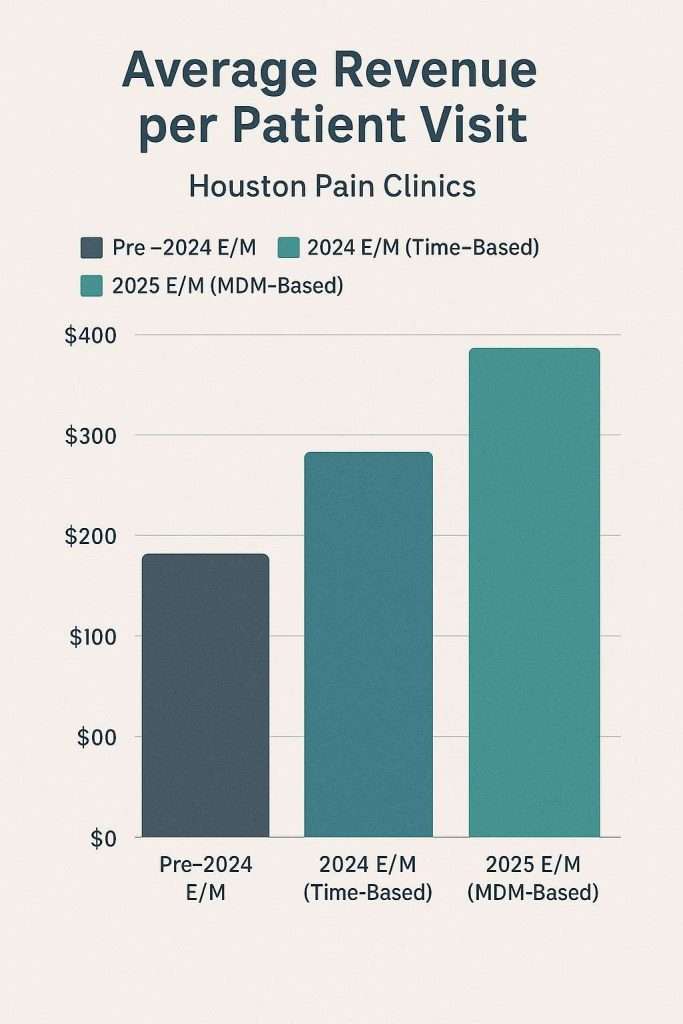
How These Changes Impact Houston Practice Revenue
The 2024-2025 E/M coding changes are not just about compliance; they have direct and significant implications for your Houston pain management practice’s revenue cycle. Misinterpreting these updates can lead to denied claims, reduced reimbursements, and increased audit risks.
Let’s consider the impact on CPT 99214 reimbursement, a commonly used code for established patient visits. Under the 2025 MDM-dominant rules, a visit that previously qualified for 99214 based on time or exam elements might now require a higher level of documented medical decision making to justify the same reimbursement. If MDM elements don’t support the 99214 level, the claim might be downcoded or denied, directly impacting your bottom line.
There are Houston-specific considerations as well. For instance, misusing a high-level code like 99205 for routine opioid management without clearly documenting the “high complexity” MDM components—such as polypharmacy, drug-drug interactions, and severe comorbidities—can trigger audits from payers. Furthermore, comparing Medicare vs. Texas Medicaid reimbursement rates reveals significant differences, necessitating precise coding that accounts for payer-specific nuances.
With 19,493 licensed physicians in the Houston region and the average pain management physician salary at $320,472, these changes demand that practices not only understand the new rules but also adapt their documentation practices to accurately reflect the complexity of care provided, ensuring maximum, compliant reimbursement.
Overcoming 3 Houston-Specific Coding Challenges
Houston’s unique healthcare landscape presents specific challenges for accurate Pain Management Billing:
1. Bilingual Documentation for Spanish-Speaking Patients
With approximately 44.1% of Houston’s population identifying as Hispanic or Latino, pain management practices frequently serve Spanish-speaking patients. Ensuring accurate and compliant documentation for these encounters, especially when interpreters are involved, requires specific protocols to avoid miscoding or audit flags. Healthcare providers must document the member’s primary language in their medical record and indicate whether interpreter services were offered and accepted or declined.
2. Telemedicine Coding Adaptations
Houston’s robust healthcare infrastructure and experience with large-scale events has shaped the region’s approach to telemedicine. The widespread adoption of telemedicine means practices must be adept at coding virtual visits accurately, adhering to evolving state and federal guidelines that can differ from in-person encounters. The 2025 CPT code set includes new telemedicine codes, though only one is currently reimbursable under Medicare.
3. Academic Medical Institution EHR Integration
Given Houston’s robust academic medical institutions like Baylor College of Medicine and UTHealth, many local practices may utilize EHR templates influenced by or directly from these systems. Ensuring these templates are updated to reflect the latest E/M guidelines, particularly for chronic pain management and interventional procedures, is crucial for compliant coding. Optimizing your EHR for efficient and accurate coding is an integral part of backoffice optimization for your practice.
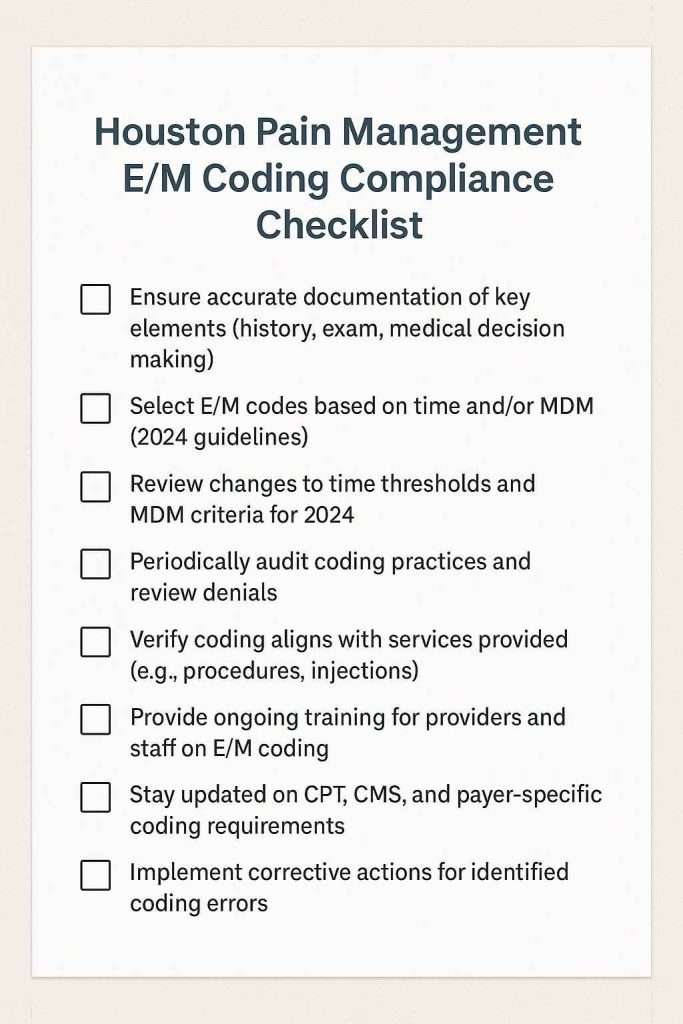
5 Actionable Steps for Houston Pain Management Coding Compliance
Proactive measures are essential to ensure your Houston pain management practice navigates the new E/M coding landscape with confidence and maintains robust revenue:
1. Audit 10% of 2024 Charts for Time Thresholds
Select a representative sample of patient charts from 2024 to assess how accurately time was documented and how effectively it translated into E/M service levels. This retrospective analysis will highlight areas where documentation practices need refinement for future time-based coding.
2. Train Staff on MDM Tiers and Documentation
With MDM becoming primary in 2025, comprehensive training for all providers and coding staff on the nuances of MDM complexity is non-negotiable. Focus on practical scenarios relevant to pain management, ensuring everyone understands how to document the number of problems, data review, and risk. These E/M Coding Changes demand a complete shift in documentation mindset.
3. Implement G2211 Tracking and Documentation Protocols
Establish clear internal guidelines for when and how to appropriately append the G2211 add-on code. Train providers on the specific documentation required to support the longitudinal, complex care criteria, maximizing legitimate reimbursement for chronic pain management.
4. Update EHR Templates with Regional Requirements
Review and revise your electronic health record (EHR) templates to ensure they align with the new E/M guidelines and any specific requirements from Texas Medicaid or other regional payers relevant to Houston. This proactive step can prevent common errors and streamline billing processes.
5. Conduct Quarterly Audits Aligned with CMS Cycles
Implement a schedule for regular, internal coding audits, ideally on a quarterly basis. Consider partnering with Houston-based coding specialists who are familiar with CMS Region 6 audit patterns and local payer nuances to preemptively identify and correct any compliance risks.
Conclusion
The 2024-2025 E/M coding updates represent a pivotal moment for pain management practices in Houston. While these changes introduce new complexities, they also present significant opportunities for financial optimization and enhanced compliance. With Houston’s position as a global healthcare leader, hosting the world’s largest medical center and treating millions of patients annually, proper coding practices are essential for maintaining this standard of excellence.
It’s crucial to acknowledge that proper coding can help offset potential audit risks by ensuring all submitted claims are meticulously accurate and fully supported by documentation. The integration of G2211 for complex longitudinal care, combined with the shift to MDM-dominant coding, provides pain management practices with tools to better capture the true complexity of chronic pain management.
Revenue protection through coding compliance and accurate billing practices
Ultimately, navigating these E/M Coding Pain Management Houston updates should be viewed not merely as a compliance task, but as a strategic initiative for growth and revenue protection. By embracing accurate documentation, continuous staff education, and proactive auditing, your practice can secure its financial health and continue providing the highest quality of care to Houston’s diverse community. For seamless adaptation to these and future coding shifts, our comprehensive Essential Backoffice Solutions for Healthcare Practices and specialized Houston medical billing and coding services are designed to support your success.

Next step
See how Synectus closes the handoff after the lead arrives.
If this article describes the exact gap inside your clinic, go one layer deeper into the service stack or book a direct strategy call with Synectus.


